Peng-Gang Xu1 ![]() ,
Xi-Feng Lei2,
Bao-Di Ren1,
Shui-Ying Lv1,
Jun-Li Zhang1
,
Xi-Feng Lei2,
Bao-Di Ren1,
Shui-Ying Lv1,
Jun-Li Zhang1
For correspondence:- Peng-Gang Xu Email: xupenggang2919@hotmail.com Tel:+865372253157
Received: 10 March 2016 Accepted: 3 January 2017 Published: 25 February 2017
Citation: Xu P, Lei X, Ren B, Lv S, Zhang J. Diclofenac transdermal patch versus the sustained release tablet: A randomized clinical trial in rheumatoid arthritic patients. Trop J Pharm Res 2017; 16(2):477-482 doi: 10.4314/tjpr.v16i2.29
© 2017 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To prepare and characterize transdermal films of diclofenac diethanolamine as a safer and more effective alternative than the sustained release (SR) tablet equivalent for prolonged relief from pain and inflammation in arthritis.
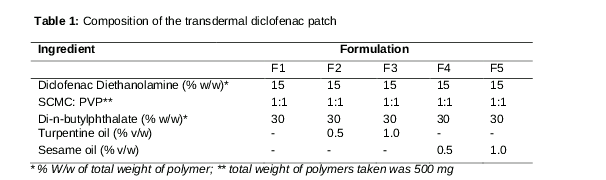
Methods: Transdermal films of diclofenac were prepared using sodium carboxymethyl cellulose and polyvinyl pyrrolidone K30, with turpentine oil and sesame oil as penetration enhancers. The films were characterized for physicochemical properties and for ex vivo permeation in a randomized clinical trial (RCT) for analgesic activities in arthritic patients.
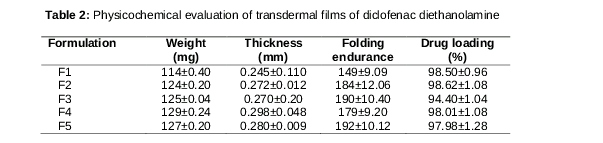
Results: The transdermal films were uniform in weight and thickness, flat, with high drug content (94.40 ± 1.04 to 98.62 ± 1.08 %) and with high folding endurance (149 ± 9.09 to 192 ± 10.12). Drug permeation through excised rat abdominal skin was prolonged. Films containing penetration enhancers showed higher ex vivo drug permeation than those without the enhancer; furthermore, drug permeation increased with increase in the concentration of enhancer. The films were non-irritating to the skin. In RCT, F3 (containing turpentine oil, 1 %v/w) decreased the pain score from 9.87 ± 1.14 to 4.94 ± 0.78 units, compared with the SR tablet (once daily) which decreased pain from 9.59 ± 0.42 to 6.49 ± 1.20 units, 48 h post-administration. Turpentine oil showed better permeation enhancement than sesame oil in the transdermal films.
Conclusion: Transdermal films of diclofenac, formulated with permeation enhancers, may have greater therapeutic advantages over conventional oral tablets in terms of prolonged release and improvement of patient compliance in rheumatoid arthritis.
Introduction
Rheumatoid arthritis (RA), an autoimmune and progressive systemic inflammatory disease, affects a huge number of people worldwide. RA adversely affects the quality of life and normal function, especially 10 years post-diagnosis. The immune system attacks joint tissues and potentially other body parts for unknown causes. RA is characteristically associated with fatigue, chronic joint pain, and prolonged stiffness (even after rest) [1,2]. Although there is no cure for RA, novel effective drugs are being explored and are available to treat the disease and prevent joint deformities [3,4]. Managing the moderate to severe chronic pain and inflammation, as well as improving the quality of life in arthritic patients, is the most challenging and important goal of anti-arthritic therapy. Non-steroidal anti-inflammatory drugs (NSAIDs) are prescribed frequently for the management of pain and local inflammation (similar to gout) [5].
Conventional oral administration of NSAIDs is associated with serious adverse effects such as gastrointestinal (GI) bleeding, renal dysfunction, blood pressure elevation, and significant plasma-drug level fluctuations, increasing the risk of overdose. Among the side effects reported, upper GI bleeding and GI toxicity are the most common [6]. Moreover, a high dosing frequency is desired for the majority of NSAIDs to provide prolonged relief from pain and inflammation.
To overcome these limitations, various novel approaches of drug delivery for NSAIDs have been investigated. Topical or transdermal drug delivery of NSAIDs is one of the most widely investigated and is a potential alternative for delivering NSAIDs. For the management of pain and inflammation in RA, localized drug delivery with polymeric dosage forms and delivery systems such as gels/creams/ointments, implants/in situ gels, and transdermal patches can deliver the drug in microenvironments of the bones, joints, or affected tissue and ligaments. The topical or transdermal drug delivery of NSAIDs has many advantages, such as localized/higher site specific delivery, prolonged drug release, avoidance of hepatic first pass, no gastric discomfort side effects, no interaction with the other drugs in multi-drug therapies, and better patient compliance [7,8]. Factors such as cytokines, prostaglandins including cyclooxygenase-2, and leukotrienes are regulated by activation of the transcription factor nuclear factor-κB and mediate pain and inflammation in RA. Therefore, any drug that can suppress the expression of tumor necrosis factor-α or suppress the activation of NF-κB may be a potential anti-arthritic drug [9].
Diclofenac is an NSAID used for the effective management of RA. Diclofenac, a carboxylic acid derivative, acts as a selective COX-2 inhibitor and is the most widely used NSAID for managing pain and inflammation after orthopedic injury/fracture, arthritis, toothache, and dysmenorrhea. Studies have reported that the efficacy of diclofenac (even at a low dosage of 100 mg/day) is as effective as other newer analgesics used in arthritis. Diclofenac shows GI irritation, peptic ulceration, and GI bleeding. Diclofenac also has a short half-life (4 h). The poor water solubility of diclofenac leads to poor dissolution and low bioavailability [10,11].
Among the various transdermal drug delivery systems, transdermal films/patches are the most recently developed dosage forms, which are well-suited for chronic pain and inflammation management of arthritic patients [12]. An ideal transdermal patch should have flexibility, elasticity, and softness. However, at the same time it must have sufficient strength to follow the body contours. It must also possess good adhesive strength for prolonged retention on the skin for the desired duration of action. The use of various permeation enhancers can improve drug flux across the skin. In addition, various chemicals are used to improve penetration across the skin, including alcohols, terpenes, and surfactants [13,14].
Therefore, the present study aims to develop and characterize transdermal films of diclofenac using two different permeation enhancers (in two different concentrations). For topical use, the diethanolamine salt of diclofenac is preferred over potassium or sodium salt. Thus, diclofenac diethanolamine was used in this report. Among the permeation enhancers, sesame oil and turpentine oil were used. The performance of the prepared films was compared with that of those without enhancer. The prepared films were characterized for various physicochemical parameters and for in vivo anti-arthritic activity.
Methods
Materials
Diclofenac diethanolamine, sodium carboxymethyl cellulose (SCMC)-low viscosity grade, polyvinyl pyrrolidone K-30 (PVP-K30), turpentine oil, sesame oil, and carrageenan were purchased from Sigma Aldrich, USA. All other chemicals were of analytical grade.
Preparation of diclofenac transdermal films
Matrix type transdermal films loaded with diclofenac were prepared using the solvent evaporation technique (). An aqueous solution of polyvinyl alcohol (4 %w/v) was used to prepare the backing membrane. The aqueous solution of polyvinyl alcohol (PVA) was poured onto flat bottom teflon molds, followed by drying at 45 °C for 3 h.
The required amount of polymers (SCMC and PVP K-30) was dissolved in distilled water with constant stirring at 300 rpm. Diclofenac (drug), propylene glycol (plasticizer), turpentine oil, and sesame oil (as permeation enhancers) were added to this solution with continuous stirring.
After uniform mixing, the solution was added to the backing membrane and kept on a flat surface. These flat bottom teflon molds containing drug-polymer solution were kept at 40 °C for 12 h in a hot air oven. The prepared cast film was cut into transdermal patches of 2 × 2 cm, packed properly, and then stored in a desiccator until further use.
Physicochemical characterization of prepared films
The films were evaluated for thickness, weigh uniformity, folding endurance, and drug content. The average thickness (of three different sites) of the film was determined using a screw-gauge in a circular cast (n = 3). The weight of each patch (5 cm2) was determined (n = 3). Folding endurance was determined by repeatedly folding a small strip (2 × 2 cm2) of film at the same point until it broke.
For the determination of drug content, the patch from each film was dissolved in 100 mL of methanol with continuous stirring for 2 h (n = 3). The solutions were filtered, diluted (100 times), and analyzed spectrophotometrically (Perkin Elmer, Lambda 25, US).
Ex vivo permeation studies
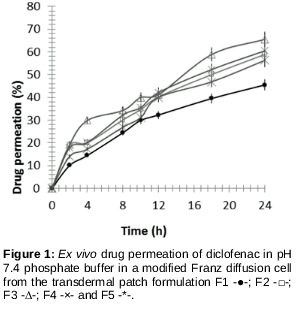
The ex vivo permeation studies of the diclofenac films were performed in a modified Franz diffusion cell through excised rat abdominal skin. A patch of 2 × 2 cm2 of each formulation was placed in close contact with excised skin. The receptor compartment of the diffusion cell was filled with 25 mL of pH 7.4 phosphate buffer. The media was maintained at 37 ± 1°C with agitation at 100 rpm. The samples (taken at different time intervals and with the same volume of fresh prewarmed media replaced in the receptor compartment) were analyzed spectrophotometrically.
In vivo studies
Healthy male Wistar rats (200250 g) were used in the studies. The rats were kept in cages standard environmental conditions of light and temperature were allowed free access to drinking water and standard diet. of the animal study were approved by the Animal Ethical Committee (approval no. 2015/4.21) and the study was according to international guidelines [15].
Primary skin irritation test
For the primary skin irritation test, healthy male Wistar rats were divided into three groups of six rats each. A 4-cm2 area of the dorsal portion of all rats was shaved and wiped with surgical spirit. The test formulation was applied over the respective test sites. The test sites were observed for any toxic side effects, erythema, and edema on the skin surface for 48 h after application in comparison to a standard irritant (2 % formalin solution) and control (blank film only).
Clinical evaluation of selected films
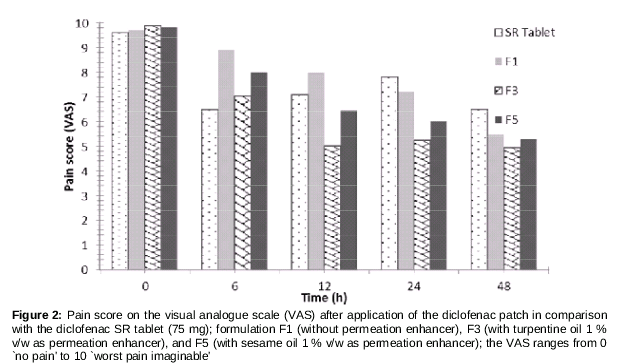
Patients in the orthopedic ward (OPD and IPD) with moderate pain due to RA were selected, and written consent of the patients was obtained for inclusion in the study. A total of 71 patients (40 male, 31 female) 49 to 65 years of age were selected for the clinical study. Three groups of 20 patients each were taken. Each group was administered one formulation (F1, F3 or F5). Eleven patients were kept on oral SR diclofenac (75 mg, po). The patients were randomized to receive drugs in a randomized crossover design, with a two-week washout period. Pain was assessed prior to treatment (baseline) and at 4, 12, 24, 48, and 72 h after administration, using a 10 point visual analogue scale (VAS, 0 `no pain' to 10 `worst pain imaginable').
Statistical analysis
The results are expressed as the mean ± standard deviation (SD) using Student’s t-test and Origin 9 software. P < 0.02 was considered statistically significant.
Results
The prepared transdermal patches of diclofenac were prepared and characterized. The effect of permeation enhancers was observed in the clinical studies.
Physicochemical characteristics of transdermal patches
The thickness, weight, folding endurance, and drug content of the prepared transdermal patches were determined (). The weight of patches (4 cm2) of different formulations ranged from 114 ± 0.40 to 132 ± 0.24 mg. All transdermal films showed uniform thickness ranging from 0.245 ± 0.110 to 0.298 ± 0.048 mm. Folding endurance ranged from 149 ± 9.09 to 192 ± 10.12. All transdermal films showed high and uniform drug content (ranging from 94.40 ± 1.04 to 98.62 ± 1.08%).
Ex vivo permeation
Ex vivo permeation across the rat abdominal skin was increased with the use of permeation enhancers (). The percent drug permeated was increased with a high proportion of permeation enhancers, with the best permeation shown by F3 (with turpentine oil). At the end of the 24 h study, the drug permeation was 45.48, 58.89, 65.54, 56.29, and 60.50 % for formulation F1, F2, F3, F4 and F5, respectively. It was evident that the permeation effect of turpentine oil was better than that of sesame oil.
Primary skin irritation
The use of the patch did not show any erythema and edema at the site of application based on primary skin irritation tests (after 48 h). Thus, the patches were considered non-irritating to the skin.
Clinical analgesic effectiveness
The VAS score of pain was studied in RA patients suffering from moderate to severe pain (pain score of 9 and above). The formulations F1, F3, and F5 were selected to study the effectiveness compared with the analgesic effect of the diclofenac sustained release (SR) tablet with VAS, which ranges from 0 `no pain' to 10 `worst pain imaginable'. The pain score decreased continuously with the formulation containing permeation enhancers (F3 and F5). F3 decreased the pain score from 9.87 ± 1.14 to 4.94 ± 0.78, while the SR tablet (once daily) decreased the pain score from 9.59 ± 0.42 to 6.49 ± 1.20, 48-h post-administration ().
It was also noted that during the initial hours of the study, the SR tablet group showed better analgesia compared with the F1, F3, and F5 groups. However, once the lag time was over and the drug started to diffuse properly across the skin, the patches group showed better activity. Moreover, the SR tablet was administered daily (once) while the patches were applied once to the subject under study.
Discussion
The topical or transdermal delivery of drugs to patients with RA is known to improve patient compliance with immediate and prolonged release of the drug [4-6]. The use of a single patch for the whole day is expected to be more patient friendly compared with frequent oral dosing of tablets. As far as drug release was concerned, the permeation enhancers or the penetration enhancers play an important role in accelerating drug release across the skin (when included in the transdermal delivery systems). Transdermal delivery of drugs can be enhanced using chemical enhancers, iontophoresis, electroporation, ultrasound, microneedles, jet injection, and thermal poration [13,14,16,17]. Of these various methods of transdermal enhancement of drug permeation, the use of chemical enhancers is the best method of increasing transport across the skin. The method is simple to adopt and cost-effective.
In this study, turpentine oil increased the permeation significantly compared with that of sesame oil. The increase was directly proportional to the concentration of turpentine oil and was in good agreement with previous studies [18-20]. Several groups have also reported turpentine oil and terpene-based enhancers as promising penetration enhancers with a greater effect on increasing the flux and anti-inflammatory activity [21,22]. The present study also found turpentine oil to be an effective penetration enhancer for transdermal drug delivery of diclofenac in the clinical study for films with penetration enhancers (F3 and F5), compared with that of films without enhancer (F1). The increasing concentration showed increased flux and increased analgesia.
The data obtained from the clinical study also supported the ex vivo permeation study results. Thus, the enhanced permeation of drug across the skin showed greater analgesic activity, thus, providing a greater benefit to those with RA.
Conclusion
The findings of this study reveal that turpentine oil and sesame oil are effective permeation enhancers in diclofenac transdermal films for use in patients with RA. However, turpentine oil is a better permeation enhancer than sesame oil. The results also show that the transdermal films of diclofenac with permeation enhancers may have greater therapeutic advantages over oral diclofenac tablets in terms of safety, prolonged release and improvement in patient compliance in RA.
Declarations
Acknowledgement
References
Archives


News Updates